-
Services
Service Directory
Direct Access
- Audiology
- Blood tests
- Cardiac Rehabilitation
- Clinics by appointment
- Local Family Health Teams
- Mental Health and Addiction Services
- MotivAction Youth Clinic
- New Brunswick Fetal Alcohol Spectrum Disorder (FASD) Centre of Excellence
- Palliative Care
- Public Health
- Respiratory Health Clinics
- Sexual Health
- Smoking Cessation Clinics
- Spiritual care
- The Single Entry Point
- Youth Services
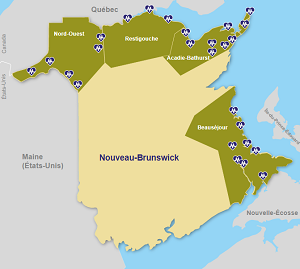
Interactive Network Map
-
Patients and Visitors
Visiting Hours
For most of our units, there is no restriction on visiting hours.
However, visitors must respect the hours of rest, from 9 p.m. to 6 a.m.
-
My Health
Chronic Illness
-
The Network
About
- Who are we
- About Our Name and Logo
- Official languages
- Research and Training
- Quality, Patient Safety and Performance Improvement
- Improvements to Vitalité Health Network's infrastructures
- Ethics at Vitalité Health Network
- Community Health Needs Assessment
- Publications
- Our partners
- Diversity, equity, inclusion, and accessibility
Administration